Disc injuries are a very common presentation to the chiropractor. We often hear a patient say they have previously had a ‘slipped disc, which sounds like a very painful injury! The good news is that it is actually not possible for the disc to slip out of place, as it held together through some very strong ligaments to the surrounding vertebra. I have detailed below some of the most common disc injuries. I also discuss a disc bulge, a very common phenomenon that does not always lead to low back pain.
In the lumbar spine, there are many different structures that can be the cause of one’s low back pain. Some of these causes can be from the vertebral joint, muscles, ligaments, nerves and the intervertebral disc. It is very important to ensure a thorough history and orthopaedic/neurological examination can help identify the cause and thus the appropriate treatment and exercises provided.
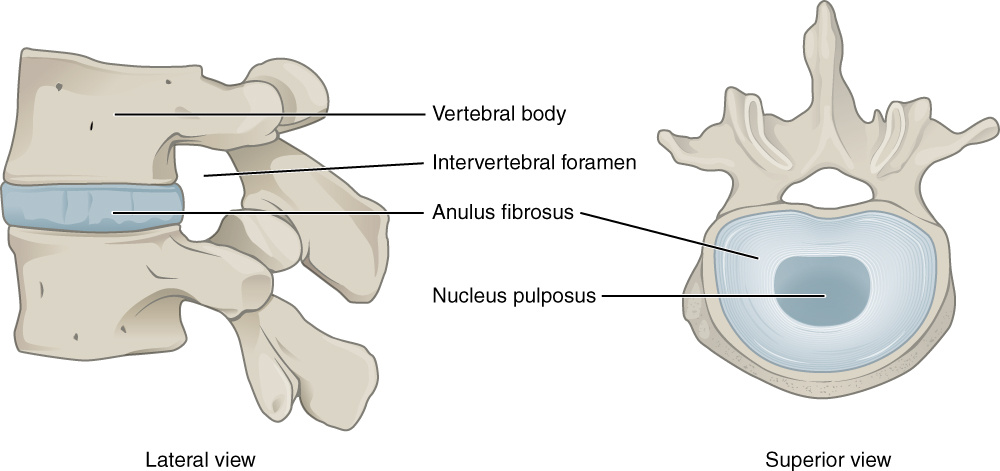
Anatomy of the intervertebral disc:
The discs are located between the vertebra and act as a shock absorber and also help distribute the load through the spine during day to day movement.
There is a total of 23 discs in the human spine – 6 in the cervical (neck), 12 in the thoracic (mid back) and 5 in the lumbar (low back). The disc is made up of a tough outer layer of cartilage (annular fibrosis) which is weaved together like a basket of 15-25 layers. The inner layer is called the nucleus pulposus, which is a gelatinous centre. (A common analogy is a jam donut. The nucleus is the jam and the outer layer is the dough).
Below, I am going to discuss a disc bulge, herniation and finally an annular tear. These definitions and classifications came about through a meeting of several professions/groups (Fardon, 2001) to clarify and standardise disc injury terminology.
Disc Bulge:
With a bulge, the structure and integrity of the disc is still intact. There is a general enlargement of the disc beyond its natural boundary although the contents of the disc are still contained.
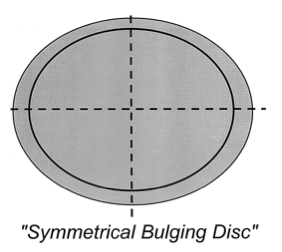
A disc bulge can often cause no pain at all. In fact, a 2015 review by Brinjikji found that in people with no back pain at all, 30% of 20 year olds had a disc bulge, with it increasing to 84% of 80 years olds having a disc bulge. A bulging disc is in fact not a diagnosis, it is more of a descriptive term for the shape of the disc contour.
So why is there such a high percentage of individuals with no back pain having disc bulges? The answer being, what structures does the disc touch, irritate or compress. Often a disc bulge is not the source of the pain, rather an incidental finding on imaging.
Disc Herniation
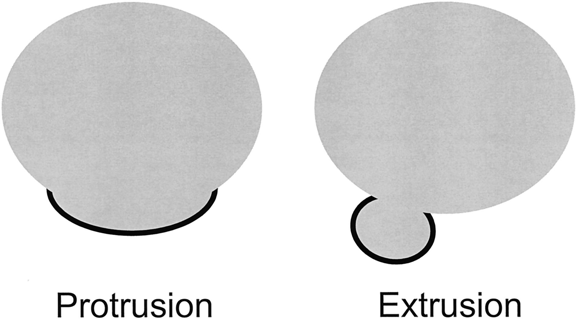
A herniation is defined as a localised displacement of disc material beyond its limits of the intervertebral disc space. Herniated discs result from damage to the tissue structure, resulting in leakage of contents. They are classified based upon their shape – either an extrusion or protrusion.
The symptoms of a herniation vary from a minor ache in the lower back and buttock, to a more severe pain that radiates down the leg, pins and needles, numbness and weakness. Often the patient leans to one side – to take pressure off that area of the disc that has herniated.
Please note that in rare circumstances, a herniation may cause a loss of control of bowel and bladder functions, which is a medical emergency.
- Protrusion – A broader base, defined as being wider that it is tall.
- Extrusion – has a thin ‘neck’ and the extruded material is longer than it is wide. A sequestration can also occur, if the extruded material breaks off at the neck.
Annular Tear
A tear can result to the outside layer of the disc, which can cause local inflammation/swelling which hence irritates the surrounding spinal nerves, resulting in sciatic pain. There is no herniation of the disc contents. It should be noted that some tears can show up on scans in asymptomatic people and thus can be an older injury that has recovered.
Do Discs heal?
The answer is yes, discs do heal and 60-90% of lumbar disc injuries can be treated with a conservative approach, such as chiropractic treatment. (Chui, et al,. 2015).
Based upon all the different type of injuries that can occur to the discs, it is important to make sure a thorough history and examination is performed. Sometimes an MRI may also be needed to show the extent of the injury and be graded. From then on, we can get a clearer picture of what the recovery time will be like for such an injury.
Mitchell Roberts – Chiropractor
References:
Brinjikji, P.H. Luetmer, B. Comstock, B.W. Bresnahan, L.E. Chen, R.A. Deyo, S. Halabi, J.A. Turner, A.L. Avins, K. James, J.T. Wald, D.F. Kallmes, J.G. Jarvik. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. American Journal of Neuroradiology Apr 2015, 36 (4) 811-816
Chiu, C. C., Chuang, T. Y., Chang, K. H., Wu, C. H., Lin, P. W., & Hsu, W. Y. (2015). The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clinical rehabilitation, 29(2), 184-195.
Fardon, D. F., & Milette, P. C. (2001). Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine, 26(5), E93-E113.